Switch language or website
Switch Language
Other countries and websites
AtlasPROfilax® is available around the world in many languages. Please select your region to switch to another website.
Technical information for health professionals about the AtlasPROfilax® method
The cranio-facial axis is the vertical axis that runs from the head to the feet. The cranio-flower deviation of the Atlas consists of a small parasagittal alteration of the position of the Atlas, a vertebra that in many cases is found in a descending direction with respect to the body, as a consequence of diverse mechanical factors.
Both conditions together, the Occipital Condylar Compression and the Cranio-Caudal Atlas Deviation are responsible for the irritation of the brain stem, the compression and angulation on one of the vertebral arteries, the congestion of the intracranial CSF, the poor vascularization of the superficial petrous nerve, the reactive muscular-fascial syndrome and the transfer of the center of gravity of the spine, from L2-L3 to L5-S1.
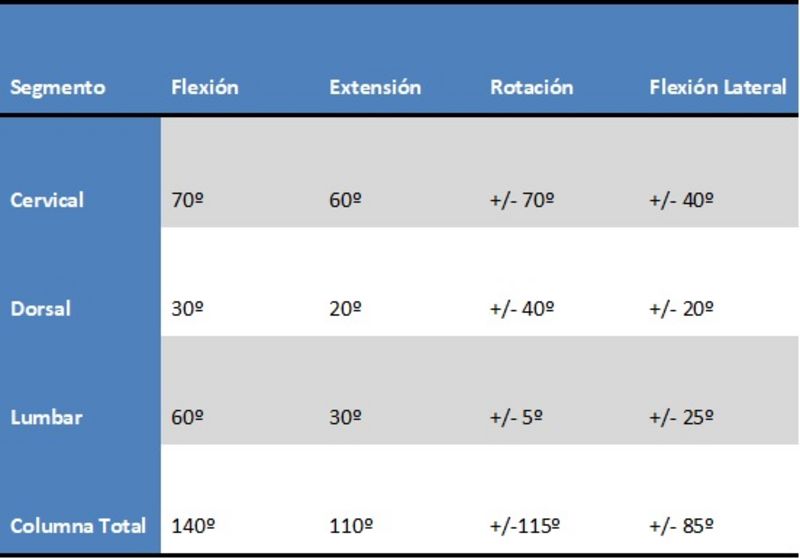
The cervical spine has to dissipate the forces acting on the head, protect the brain stem and the nerves and blood vessels that travel through it. Its joint system has three joint systems: Anterior (intersomatic-uncovertebral) and two posterior (zygapophyseal). Its range of motion is very high and the disc diameter is relatively small.
The thoracic spine must protect the medullar axis and provide the statics of the trunk. The discs have similar height and smaller diameter than in the cervical or lumbar region. The stability of this area is given by the attachment of some dorsal vertebrae to the ribs and muscles. It is especially the yellow ligaments that resist the tensile forces of this segment.
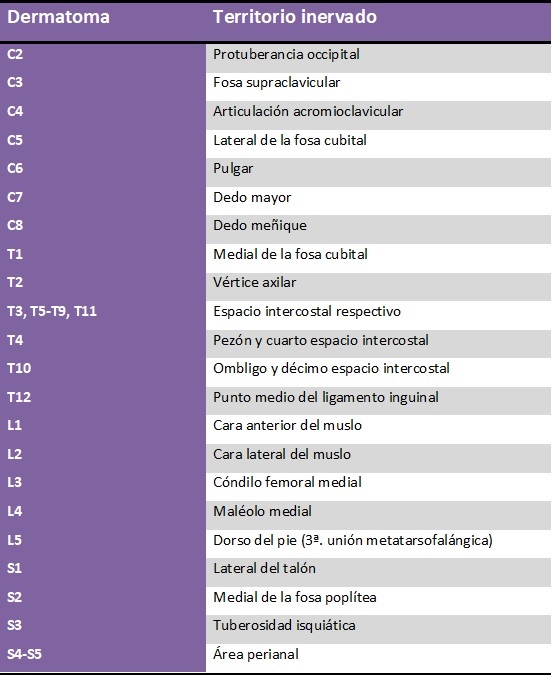
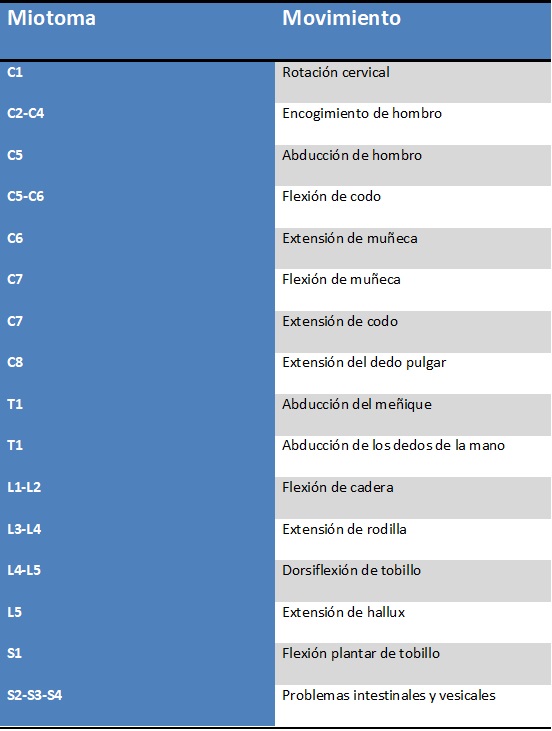
The innervated skin area that carries sensitive information to a root is called a dermatome, the muscle group innervated by a single spinal segment is known as a myotome, and the skeletal area innervated by a segment of the spine is called a sclerotome. For each metalmere there is a segment of the spine, a dermatome, a myotome, and a sclerotome.
As a rule, the number of dermatomes is equal to the number of spinal segments. However, C1 is the exception in that it has no cutaneous territory. Thanks to the maps that have been developed for the location of dermatomes, it is possible to make neurological diagnoses to detect spinal cord and CNS lesions.
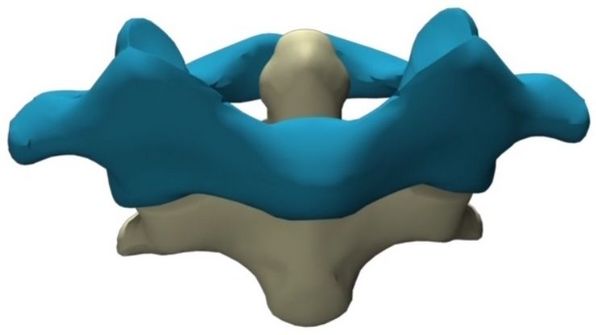
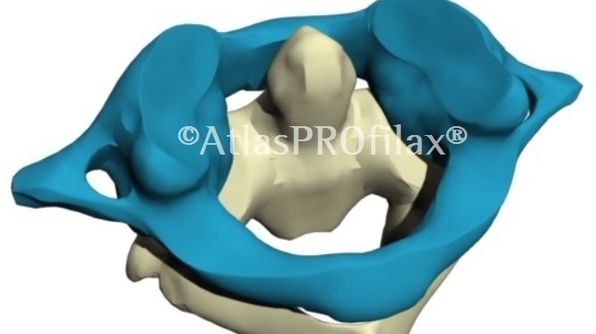
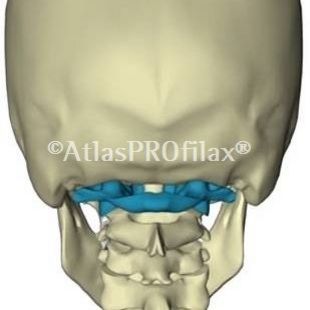
The upper face or glenoid cavity is articulated with the occipital condyle, thus forming the atlantooccipital joint, which consists of a bicondile diarthrosis formed by condyles of C0 - lateral masses of C1 and fixed by capsules, membranes and atlantooccipital ligaments. Its function is the flexion, circumduction, extension and lateralization of the head, with very little rotation.
The C1-C2 joint is created between the inferior veneers of the lateral masses of the Atlas and the superior veneers of the Axis (atlantoaxial) or between the anterior arch of the Atlas and the dens of the Axis (atlantoodontoid). It is the transverse ligament of the Atlas that maintains this joint identity. One third of the internal area of the Atlas is occupied by the dense, another third by the transverse ligament and the last one by the spinal cord.
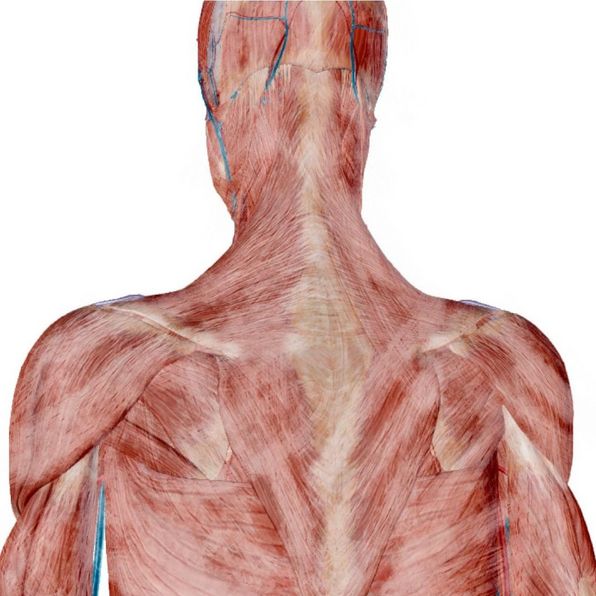
In the posterior tuber of the Atlas, the posterior minor rectus of the head is inserted; in the anterior tuber and arch, the length of the neck and the anterior minor rectus of the head are inserted while the transverse processes of the Atlas serve as insertion surface for the oblique of the head, lateral rectus, scapula elevator, posterior scalene, cervical splenius, intertransverse of the neck and transverse spinous.
The final goal of AtlasPROfilax, when carrying out this integration, is to recover the biodynamic balance of the human being as it reduces the stress of the suboccipital muscles. This translates into:
Mechanical vibropressure has been calculated based on two laws of biophysics that are useful for fascial work. They are:
Arndt-Schultz's Law: SWeak stimuli excite physiological activity, moderately strong ones favour it, strong ones delay it and very strong ones block it.
Hilton's Law: It is related to the capacity of the nerve - which innervates a joint - to innervate also the muscles that mobilize this joint, as well as the skin that covers the joint insertion of these muscles.
The suppression of the stress of the suboccipital muscles can also result: