Switch language or website
Switch Language
Other countries and websites
AtlasPROfilax® is available around the world in many languages. Please select your region to switch to another website.
Technical information for health professionals about the AtlasPROfilax® method
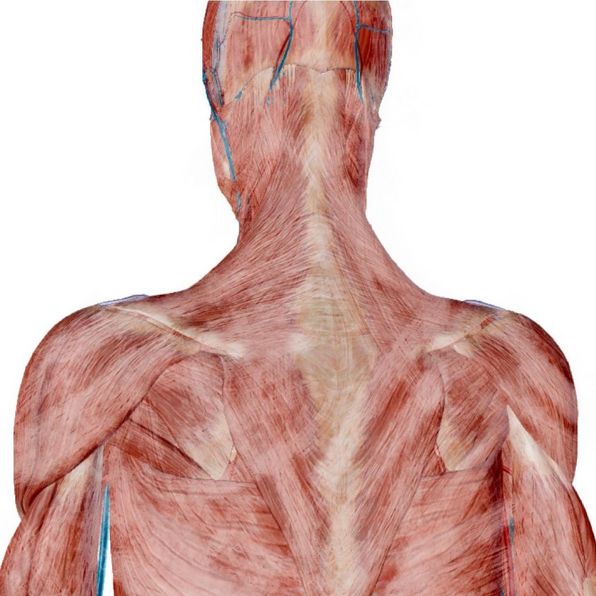
A healthy fascial system allows the different organs to glide over each other to allow a correct functional development. For example, the fascia of a muscle allows it to slide over the other muscles during contraction. The sliding of the pleura allows the expansion of the lungs and the rib cage by allowing the structures to move over each other. When the fascial system is unhealthy, mobility restrictions occur, which, due to the continuous nature of the fascial system, may affect the function of other organs located at a distance.
Functionally, the fascial system also includes the meninges, and the dura mater is the most important membrane due to its characteristics (greater thickness and less elastic capacity). Some authors call the meninges the Internal Fascial System and the rest of the fascial system the External Fascial System.
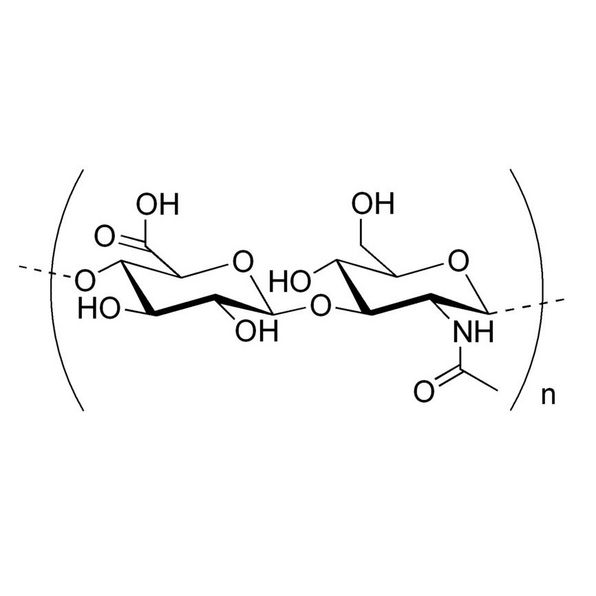
The third component of the connective tissue is the set of cells, divided into two groups: fixed cells and free cells. Among the former are fibroblasts, whose function is to produce elastin and collagen, and adipose cells, whose function is to store lipids and then release them into the blood for energy.
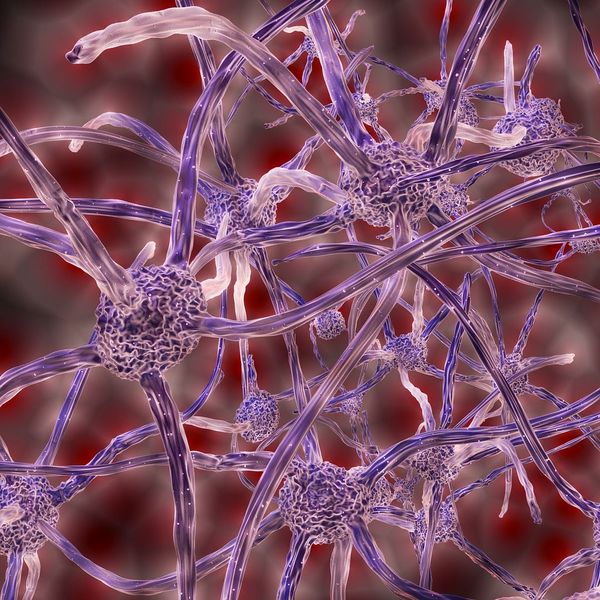
As for the free cells we can find macrophages, which "eat" the damaged cells and other waste substances when there is an injury and participate in the process of repairing damaged tissue, and mast cells, which participate in the task of renewing the fundamental substance, since their function is to release certain substances necessary for the repair or healing process, particularly produce histamines, serotonin and heparin in the early stages of the inflammatory response.
Within the deep fascia, different levels are established:
Starting from the existence of the fascial system capable of integrating each structure of the body, whether at a microscopic or macroscopic level, different therapeutic currents are born which have the common objective of understanding the organism as a whole and having a new vision of the pathology, which is based on the macroscopic but also cellular restriction and deformation of the fascial system, in order to develop effective liberation techniques capable of restoring the body's capacity for movement and consequently recovering health.
Although each of these currents has certain theoretical principles about pathogenesis and therapeutic action, all of them nourish the theoretical principles of the AtlasPROfilax® method, which far from entering into theoretical or dogmatic discussions, has been able to take the essence of each of them and integrate them in order to better understand the great therapeutic potential of the method itself.
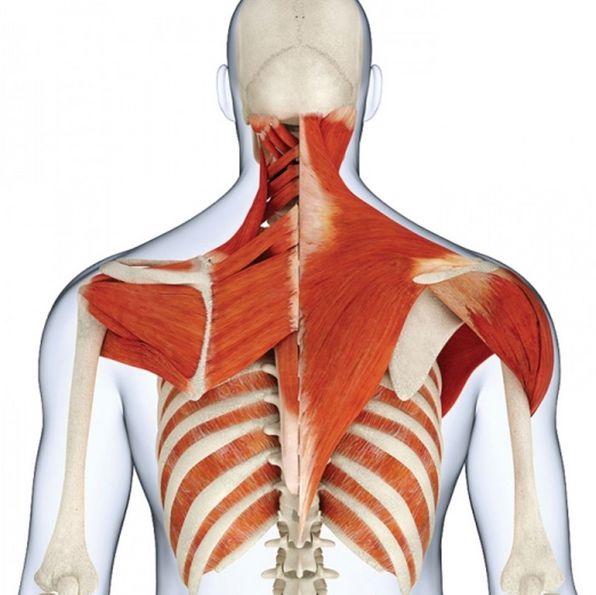
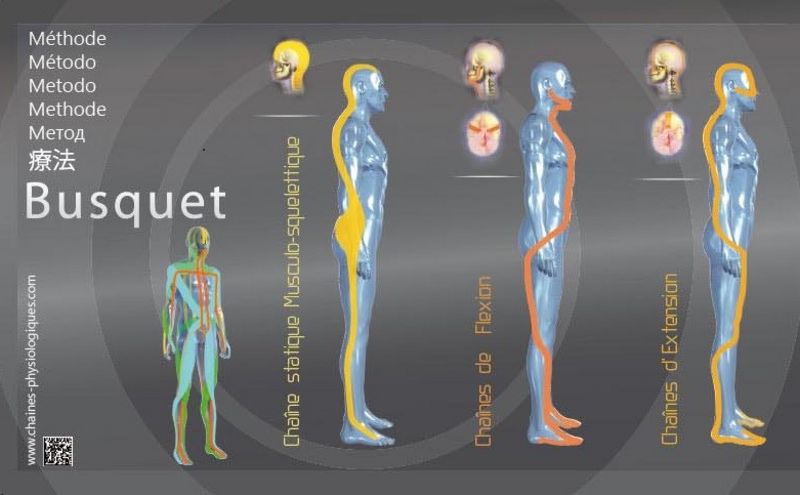
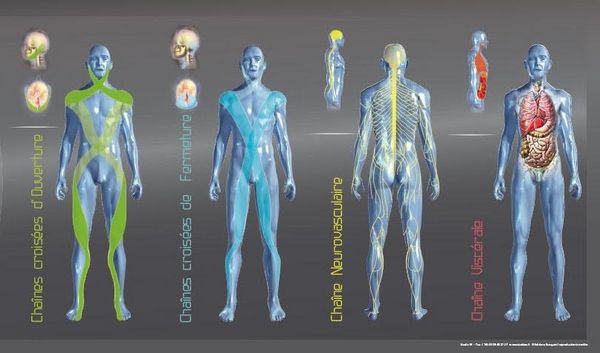
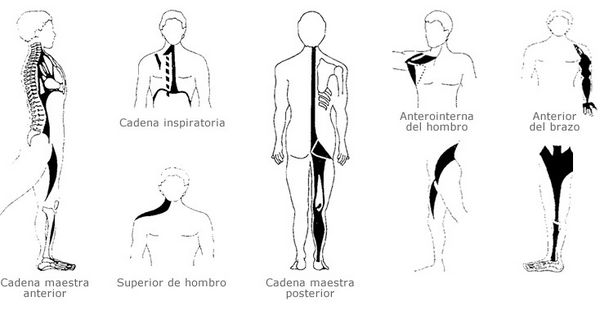
Leopold Busquets adds some interesting notions such as the inclusion of the dura mater and the visceral fascia. He also establishes the existence of a posterior static chain (PSC), which he considers to be formed by elements of connective tissue such as the cerebral falx, the nuchal septum and the thoracolumbar fascia among others, but he also establishes two other static chains, visceral and neurovascular, thus giving great importance to the connective or fascial tissue as opposed to the muscular tissue. It also considers that there are some dynamic chains involving flexion, extension, opening and closing.
Images of muscle chains taken from L. Busquets. In yellow the CEP and the neurovascular C. and in red the visceral C., in orange the flexion and extension C., in green the opening C. and in blue the closing C.
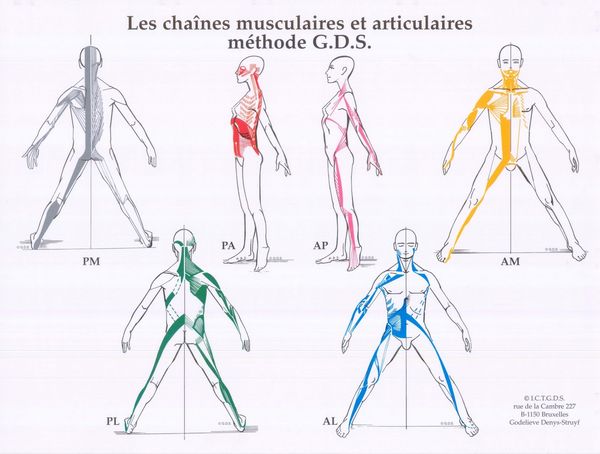
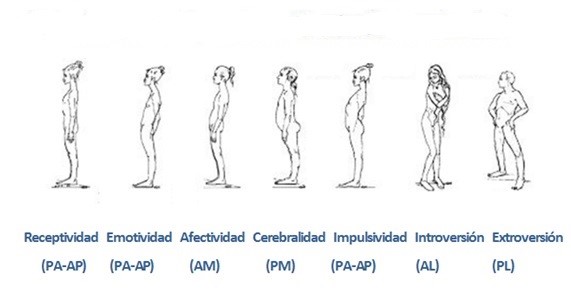
Other authors such as J. Pilates, Ida Rolf, Thérese Bertherat, Alexander point out various approaches and interrelations of the myofascial system. For example, Godelieve Denys-Struyf, talks about the relationship between mechanics and body statics with psychological aspects. This author states that the function of the body is to express the psychological aspects of the person. She also introduces the term joint chain, as a set of joints that act in a coordinated way in the different movements. The muscle chains sit on the joint chains and are the motor of the joints.
Given the above, we can draw different conclusions. Firstly, the existence of static and dynamic myofascial chains, with the static ones being responsible for the posture. These myofascial chains possess a large amount of connective tissue that is more effective than muscle tissue for this purpose.
Although there are great methodological differences between different authors not mentioned here for practical reasons, there is consensus between all of them on some points. On the one hand, they all agree on the importance of the fascias in the whole system and that shortening one part of the chain has an impact on the whole chain. Furthermore, if we look at the static chains in each of them, they are born or have a critical point in the craniospinal junction.
From the point of view of the AtlasPROfilax® method we can state that the knowledge of the myofascial chains allows us to understand in a large percentage how and why such important and rapid changes in the posture of our patients occur and why joint mobility is restored and pain reduced within a few days or weeks of the AtlasPROfilax® treatment, even after suffering significant restrictions and deformations. The elimination of the Reactive Syndrome of the Suboccipital Muscles, the decompression of fascial structures with biochemical changes in the atlanto-occipital hinge area releases the muscle chains producing a great physical and psychic benefit on the organism of our patients.