Switch language or website
Switch Language
Other countries and websites
AtlasPROfilax® is available around the world in many languages. Please select your region to switch to another website.
Specialists from disciplines not initially related to dentistry, such as A. Pilat, M. Rocabado or Chaitow, have done an excellent job in which they highlight the need to address many cranio-mandibular disorders by expanding the focus and therapeutic approach to Occipital-Atlas-Axis and the biomechanical interactions of the soft tissues, especially the fasciae and their tensegritic behavior with the rest of the connective tissues. The latest therapeutic trends in dentistry underline the need for a kind of marriage when dealing with many dysfunctions that are difficult to resolve or easily relapsed in classic dental and orthopedic-maxillary treatments.
Atlas repositioning with AtlasPROfilax® provides convincing explanations for the cause and persistence of these disorders and offers a valid solution for the treatment of these dysfunctions, establishing itself as a very useful complementary and adjuvant method in the treatment of cranio-cervical and craniomandibular dysfunctions.
The proprioception of the spine, ocular motricity and plantar support are interrelated with the inner ear forming a complex integrative system that maintains (or distorts, if dysfunctional) the correct muscle tone that results in the maintenance of posture and body dynamics.
At the level of sensory afferents, the receptors are classified as follows:
Primary:
Secondary:
The tonic balance between the anterior and posterior muscle chains is key to understanding the correct or pathologically adaptive functioning of the PTS. There are a large number of very diverse elements involved in the balance of the PTS that can be related to compensation or decompensation of the tone of the anterior and posterior muscle chains.
The relationship between the anterior and posterior musculature is manifested in:
Elements external to the stomatognathic system can cause auditory and visual disturbances, vertigo, headaches, nausea, nystagmus, swallowing disorders and TMJ dysfunctions.
Recent research in the field of neuroscience indicates that the regulation of the postural system is far from being exclusively regulated by the inner ear. The feet, the eye and above all proprioceptors in certain muscles play a role as or more important than the inner ear.
Dysfunctions in the main proprioceptive receptors lead to a dysregulation of the Postural Tonic System leading to important alterations not only in posture but also in the locomotor system.
There are also other postural sensors such as the chewing apparatus and the presence of scars. The body tends by compensation and adaptation to generate adaptive mechanisms that will integrate as "normal" the dysfunction of the Postural Tonic System creating adaptive mechanisms that usually lead to very diverse pathologies with the passage of time. The body, therefore, is able to continue functioning within the "imbalance" although sooner or later, it will pay the consequences (attention deficit, mouth breathing, vertigo, headaches, muscle pain, among many others).
Thus, the entire trigemino-cervical complex may comprise the C1-C4 and cranial nerves V, VII, IX, X, XI and XII. The extensive sensory and motor innervation represents the most important source of efferent control in the entire cranial and suboccipital region.
Anteriorization of the head modifies neural information and changes the biomechanics of the cervical spine in general. Temporo-Mandibular Dysfunction is usually the result of sustained mechanical dysfunction of the cephalic axis altering all of the body's own defense and correction mechanisms.
In all these cases, osteopathy and kinesiology sessions are highly recommended to slowly lead to a correction of the muscular imbalance of the system by soft tissue manipulation. However, if there is a profound mechanical alteration at the level of the atlanto-occipital joint, it is first necessary to resolve this profound blockage.
The masticatory muscles have been shown to have electromyographic occlusion changes due to leg length discrepancies. Loss of lumbar lordosis, which is commonly due to sitting or working with the forehead tilted forward, causes frontal cephalic stoop. The center of gravity of the skull is located at the bisection of the vestibular apparatus of the inner ear. Hyperextension causes reflex defense of the anterior muscles, e.g., the long neck, sternocleidomastoid and scalene muscles, resulting in a forward tilt of the head. The concomitant hyperflexion produces reflex defense of the short suboccipital extensors, upper trapezius and angularis scapulae.
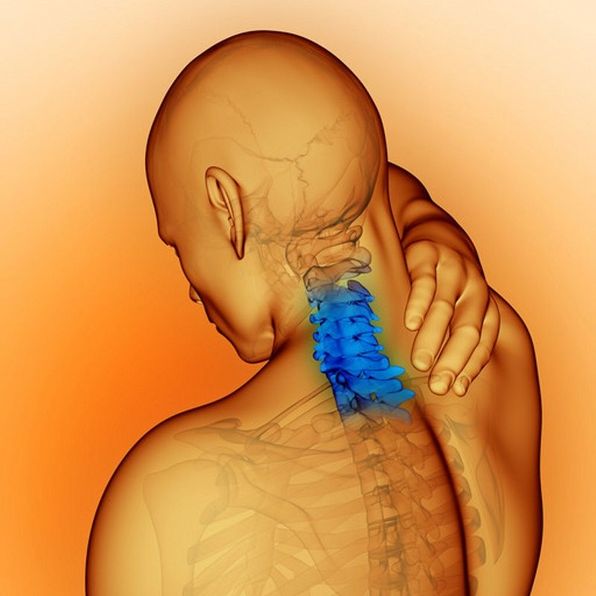
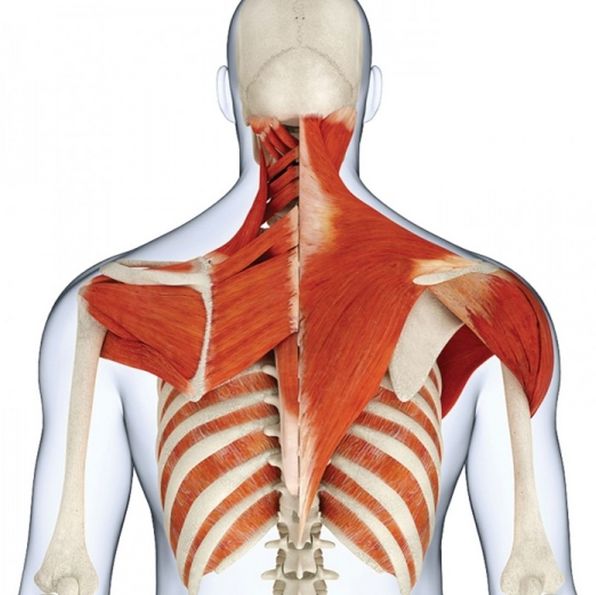
The forward position of the head converts the suboccipital kyphosis into lordosis, bringing the occiput, atlas and axis closer together, thus causing a suboccipital compression that may affect the trigeminal-cervical complex and the vertebral artery. When there is also posterior cranial rotation, the compressive force is accentuated. The occiput approaches the shoulder girdle and the upper trapezius and angular trapezius scapulae muscles are shortened. The middle trapezius, lower trapezius and rhomboids distend, resulting in forward displacement, internal rotation of the glenohumeral joint and compression of the sternoclavicular and acromioclavicular joints, with concomitant shortening of the pectoralis muscles. The temporalis muscle may contract the mandibular elevators and cause mandibular elevation and retrusion.
Segmental facilitation can have several origins: mechanical, metabolic, emotional or somatic. In all cases the muscle is affected in its normal length and viscoelasticity, increasing the level of toxins and metabolic wastes in the cytoskeleton and affecting regionally or distally other regions of the body. Such alteration sustained over time leads to an alteration of nociceptive and proprioceptive signals traveling to the thalamus.
Some studies have shown that the masticatory muscles can be affected by electromyographic signals in occlusion due to pelvic tilt, retraction of the ischiosural musculature and the existence of a functional short leg.
Anteriorization of the head favors cervical lordosis at the suboccipital level "bringing together" C0-C1 and C2 and producing a suboccipital compression that will involve the vertebral and trigeminal-cervical complex. If there is posterior cranial rotation, the compression increases and the occiput will approach the shoulder girdle thus shortening the upper trapezius and scapula angularis. On the other hand, the middle trapezius, lower trapezius and rhomboids deform producing an internal rotation of the glenohumeral joint and compressing the sternoclavicular and acromioclavicular joints, thus shortening the pectoralis muscles. In turn, the temporalis muscle will tend to shorten the mandibular elevators causing mandibular elevation and retrusion.
Atlas mechanical dysfunction - or Minor Intervertebral Disarray (MID) - feeds back into the dysfunctional cycle of Upper Cross Syndrome and often perpetuates and aggravates pathomechanical conditions by creating primary downward spreading lesions and secondary upward spreading lesions. A knee pain could be the consequence of an ascending injury originating from the talus, for example. But talar dysfunction could in turn be a consequence of a descending injury from the TMJ whose ultimate mechanical cause could very well be the Atlas MID.
Among the problems associated with upper crossed syndrome we find TMJ dysfunctions with very varied symptomatology.
Although several causes of different nature (psychological, metabolic, nutritional, traumatic) can coexist, the Minor Atlas Intervertebral Disarrangement is usually one of the most primary and common causes in the development and perpetuation of the Upper Crossed Syndrome with all its pathological derivations from the TMJ to the support of the feet.
Authors such as Brodie, Huggare, Goldstein and Makofsky have highlighted in the existing literature the interrelationship between the position of the head and cranio mandibular structures and their determining influence on head and neck posture. If we consider the human body and its vast connective tissue as a system or global model of tensegrity, we can affirm that the influence of the cranio mandibular structures and, in particular, the position of the Atlas, are determinant for the entire posture of the human body: from the shoulder girdle and pelvic girdle to the pronation of the knees or ankles and the final support of the feet.
A study conducted at the London Medical Center (England) by Dr. Matthew Voigts, Doctor of Osteopathy, on 350 patients with functional short leg showed that, after correction of the Atlas with AtlasPROfilax®, the functional short leg disappeared in 90% of the subjects studied, and the pelvis position was also normalized. In the remaining 10% of patients, an improvement of the pelvic position and shortening of the shortened lower limb was observed, without, however, reaching full normalization. No case was found in that study that any of the 350 patients had remained without positive changes, partial or total, in the perfect alignment of the pelvis or of the functional short leg. Although AtlasPROfilax® is performed in a single session without the need for subsequent adjustments with the same therapy, the study showed that the changes and improvements were maintained over two and a half years, unlike other osteopathic, kinesiolologic or chiropractic treatments where relapses are very common, despite the benefits of these therapies.
This syndrome is responsible for the persistence and recurrence of cervical and TMJ problems despite classic orthopedic-maxillary treatment because it causes the brain to send distorted signals to muscles and fasciae, causing them to alter their length and viscoelasticity, deregulating the body's tonic-postural, nociceptive and proprioceptive systems.
Although classical dentistry has had difficulties in finding effective and lasting treatments for these problems, in recent years kinesiology and osteopathy have joined hands with dentistry to find more effective and lasting treatments for craniovertebral and TMJ problems.
In this sense AtlasPROfilax® provides a unique complementary and supportive tool to all those dentists and kinesiologists focused on the treatment of temporomandibular dysfunction and related pathologies.
AltasPROfilax® corrects in one session the pathomechanical dysfunction of the C0-C1 joint while greatly improving or suppressing the Reactive Syndrome of the Suboccipital Musculature, standing as a primary and highly recommended therapy prior to any orthopedic, orthodontic or dental treatment.
Part of the arterial irrigation systems of the dura mater are usually "pressed" by the mechanical disarrangement of the cranio-spinal junction. The result is poor irrigation at the level of the C3 vertebra that contacts the hyoid through the stylohyoid ligament, affecting the temporal bones and the hyoid. This negative feedback results in an even greater increase of the temporomandibular musculature.
The excessive amount of fribroblasts in the connective tissue generates a shortening of the muscles by almost half, affecting the extracellular matrix and the stroma, producing an excess of tension in the bone and in the TMJ, as well as in all the surrounding musculoskeletal structures. The body's defense mechanism to relieve this tension is an involuntary movement of the jaw causing bruxism or teeth grinding.
This defense mechanism to the attack of fibroblasts that the muscles are suffering as a consequence of the irritation of the mandibular style is not only a product of the decompensation between both posterior muscular chains. The vicious circle that the Atlas MID produces and perpetuates mechanically in the suboccipital musculature, further affecting the posterior and anterior chains and transferring the problem to the lateral muscles, is very often at the root of the problem.
Bruxism of emotional or psychological origin has to do with traumatic events, especially in childhood, very often related to very authoritarian or abusive parents. The person represses anger by accumulating it in the jaw area.
This type of bruxism depends on the emotional state and the adrenal glands together with the stress axis (HHS). A high incidence has also been found in certain women with hormonal disorders and ovarian problems. Although AtlasPROfilax® improves in some cases the stress and some of the temperament by disinterference of the nervous system and can even produce profound emotional changes with the revival and healing of old psychological traumas, this does not happen in all cases. For this reason, if the origin of bruxism is emotional, psychological or hormonal, the incidence of AtlasPROfilax® in its improvement will be low or very low. Structural or functional bruxism is related to the length or viscoelasticity of the muscles in both the anterior and posterior chain. The anterior and posterior chain in the neck are used a lot for the cephalic movement. This musculature is subjected to so much work and solicitation that one of the two chains tends to alter before the other, with the MID of the Atlas usually being the main mechanical alteration. In people who bruxate, the anterior muscular chain is usually compromised first (similar to what happens with cervical rectification), suffering from hypertonicity. The long neck, lateral rectus, digastric and mylohyoid muscles usually have an excess of tone in the anterior area in these cases.
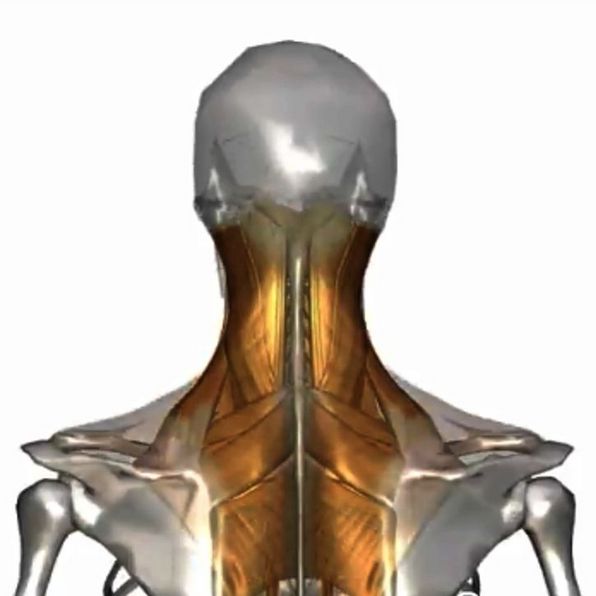
The persistence of a C0-C1 MID leads to an excess of tone in the suboccipital musculature from C0 to C2. This excess tone, together with that of the anterior chain, causes all the lateral neck muscles (platysma, lateral rectus, levator) to become involved, especially the stylomandibular ligament. The involvement of this ligament tends to produce inflammation and irritation, and this permanent state causes the nerve fibers to transmit erroneous nociceptive and proprioceptive signals to the medulla creating a general distortion in the position of the head and position of the mandible.
The distorted nociceptive signals traveling through the thalamus to the higher centers and the reticular formation - and to a lesser degree the tonsil - cause the brain to release large numbers of attack cells generating fibroblasts in the masseters and pterygoids which are highly stressed muscles (e.g. by speech).
AtlasPROfilax® has proven to be a useful tool in the prevention of part of the temporo-mandibular dysfunctions while being able to eliminate or substantially reduce the symptomatology and pain associated with cranio-cervical and temporo-mandibular dysfunctions.
Listed below are indications for AtlasPROfilax® as a useful therapeutic tool in the elimination or reduction of pain and cranio-cervico-mandibular dysfunctions. It should be noted that, like many therapies, there are certain limitations in which the therapy will not have a notable incidence in the resolution of the pathologies.
HIGH INCIDENCE IN
LOW INCIDENCE IN
"¡Se me quitaron los dolores!"
"¡Mi vida cambió! ¡Volví a nacer!"
Odontóloga nos cuenta su experiencia con AtlasPROfilax. "¡En este momento soy otra persona!"