Switch language or website
Switch Language
Other countries and websites
AtlasPROfilax® is available around the world in many languages. Please select your region to switch to another website.
Information on Minor Intervertebral Derangement of the Atlas
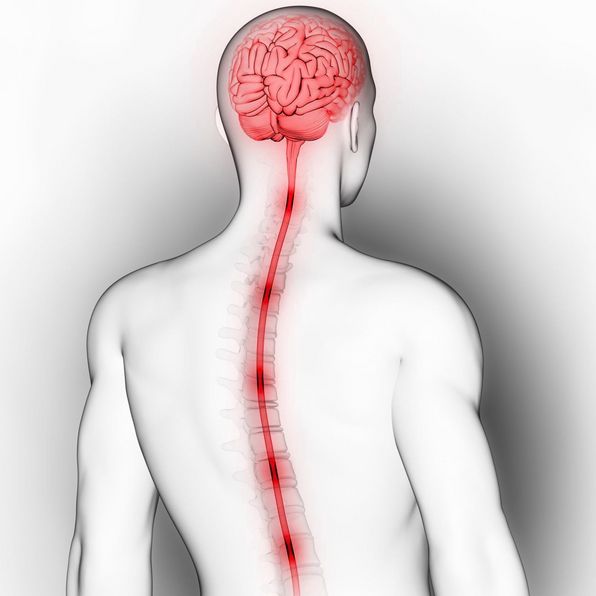
The irregular fit of the occipital condyle in the glenoid cavity of the Atlas can have mild to devastating consequences as the hydraulic force of the cerebrospinal fluid (CSF) is affected. In addition, it increases the tendency to occipital and temporal bones tension that in children, is usually registered as headache and learning difficulties.
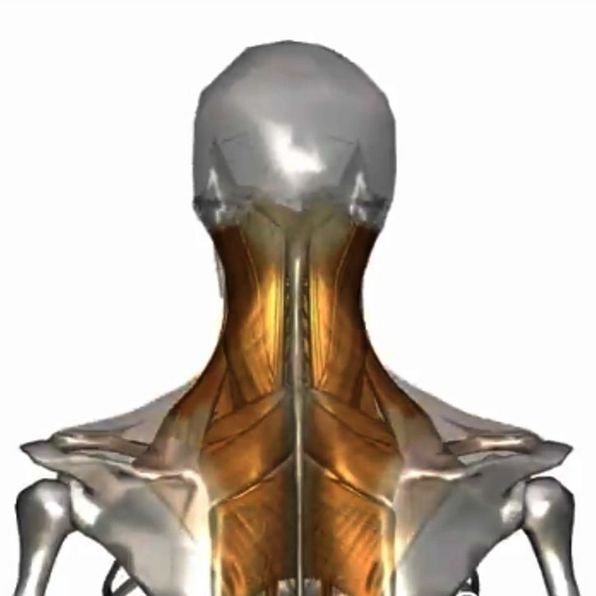
Due to the longitudinal fascia, the muscle chains are pulled downwards along the body. The plastic deformation of the fascia leads to possible irregularities in the stomatognathic apparatus, which induce a change in the cephalopodal axis and therefore modify the loads to which the intervertebral discs are subjected, especially those of the lumbar segment.
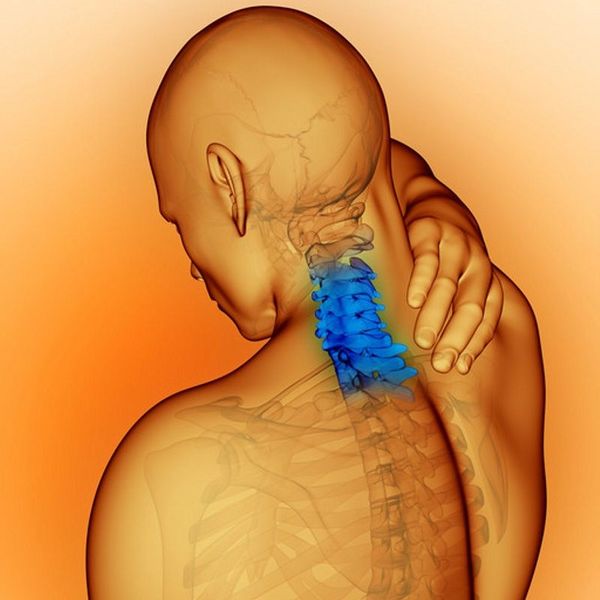
As the anchorage between the occipital bone and the atlas is slightly unstructured and compressed, this condition basically has repercussions on three levels. They are:
Often, compression of the occipital condyls on the surface of the Atlas leads to excess tension in the sphenoid (skull bone), which can worsen headaches ( cephalea), muscle stiffness and tension (spasticity), and learning problems (speech, reading, and reasoning difficulties), which often become chronic.